Abstract
The incidence of breast cancer in women is on the rise worldwide, including in developing countries. The objective of this study was to describe the epidemiological, clinical, and histological characteristics of breast cancer in women in Mauritania. Data were collected from 60 female patients monitored and treated at the National Hospital Center (NHC) and Military Hospital Center (MHC) in Nouakchott. The variables studied were age, parity, age at first pregnancy and menarche, place of residence, socioeconomic status, medical coverage, tumor site, Scarff Bloom and Richardson histoprognostic grade, location, Tumor Nodes Metastasis stage, molecular phenotype, and lymph node involvement. The average patient age was 48.71 ± 12.45 years, ranging from 17 to 70 years. Regarding histological types, invasive ductal carcinoma was the most frequently encountered (70% of cases). Immunohistochemical profile analysis revealed that 44% of the tumors were luminal A type, 24% were triple-negative type, and 22% were luminal B type. Our results also revealed that smoking patients had more grade III tumors, and that age was significantly correlated with disease stage (p=0.047) and molecular classification (p=0.0011). The characteristics of breast cancer in Mauritania do not differ from those in other developing countries.
Keywords
Cancer, Breast, Epidemiology, Mauritania
Introduction
Cancer is a major public health problem, and according to the World Health Organization, it is the second leading cause of death worldwide, causing 8.8 million deaths in 2015. Nearly one in six deaths worldwide are due to cancer. According to the latest WHO estimates, the number of cancer deaths is expected to continue to rise, and to exceed 11 million people per year by 2030.
Breast cancer is the most common malignant tumor type in women worldwide, and its incidence continues to increase, particularly in the 35-55 age group [1]. Mauritania ranks first in terms of breast cancer incidence and mortality among women [2]. According to some studies [3,4], this pathology is indeed the first cancer in women, although its frequency varies according to ethnicity, and it remains a major source of female mortality, as diagnoses are usually made at an advanced stage.
Several risk factors for the development of breast cancer have been recognized, including family history of breast cancer, advanced age, early puberty, late menopause, nulliparity, and obesity. However, no factor directly linked to its onset has been identified, except for the hereditary transmission of the BRCA 1 and 2 genes, which have been implicated in 5-10% of cases of breast cancer cases since Bittner’s discovery. In addition, many viruses are suspected to cause breast cancer [5]. This prospective study aimed to highlight the epidemiological, clinical, and histological characteristics of breast cancer in Mauritanian women.
Methods and Materials
This is a descriptive study of sixty patients. The study included patients newly admitted to the National Hospital Centers (NHC) and Military Hospital Centers (MHC) in Nouakchott for the treatment of breast cancer. All histologically confirmed malignant breast tumors were included in this study. The following variables were studied: age, parity, age at first pregnancy and menarche, place of residence, socioeconomic status, medical coverage, tumor site, Scarff Bloom and Richardson histoprognostic grade, location, TNM stage, molecular phenotype, and lymph node involvement. The data were collected by consulting hospitalization records, which are kept in the archives on a pre-established sheet. Data entry and analyses were performed using Microsoft Office Excel and RStudio, respectively. Correlations between certain factors, such as the grade, stage, presence or absence of metastasis, molecular classification, tobacco consumption, and patient age were analyzed in this study. In particular, the presence of a relationship between grade and tobacco consumption was investigated.
Results
Sixty patients with breast cancer were included in this study. The average age was 48.71 ± 12.45 years, ranging from 17-70 years. The average age of menarche was 12.66 ± 1.21 years, ranging from 11-16 years. The mean age at first pregnancy was 21.89 ± 3.02. The average number of births was 1.32 ± 0.60. Two of the patients were nulliparous. Overall, 43.33% were White Moors, 35% were Black Moors, 10% were Fulani, 8.33% were Wolof, and 3.33% were Soninke. A total of 53.33% of patients lived in rural areas; 71.66% of the patients were married, and 81.66% had a low socioeconomic level. A total of 56.66% of women had no social security coverage, and 11.66% of the patients were smokers. Only 5% of the patients were physically active, and 93.33% of patients had palpable nodules.
In our series, the most marked clinical tumor size according to the TNM classification was T2 (74,98%) (Figure 1). Of the tumors, 65% were stage IIA and 28.33% were stage IIB (Figure 2). The SBR grade II was the most represented in our series (73.33%) (Figure 3). The right breast alone was the most frequently affected (58.33%), followed by the left breast alone (36.66%), and bilateral location (5%).
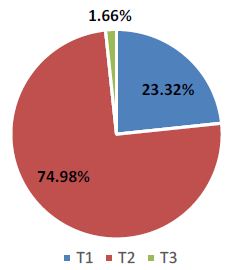
Figure 1: Distribution of cases by TNM classification
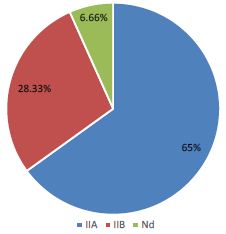
Figure 2: Distribution of cases by disease stage
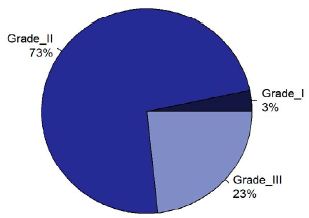
Figure 3: Distribution of cases according to grade
Histological analysis showed that invasive ductal carcinoma (70% of cases) was the most frequent type (Table 1). Regarding immunohistochemical profiles, the analysis revealed that 44% of the tumors were luminal A type, 24% triple-negative type, and 22% luminal B type (Table 2). Of these patients, 51.33% had undergone chemotherapy. Local recurrence was observed in 41.66% of patients and regional recurrence in 1.66% of patients. Of these patients, 16.66% presented with metastasis. 97% of patients are alive during hospitalization (Figure 4).
Table 1: Case distribution according to histological groups
|
Histology |
Adenofibroma |
IC |
DC |
NSC |
SC |
MC |
DC (L) |
PC |
DC (R) |
| Number |
1 |
1 |
2 |
6 |
1 |
1 |
42 |
5 |
1 |
| Frequency |
1.66 |
1.66 |
3.33 |
10 |
1.66 |
1.66 |
70 |
8.33 |
1.66 |
IC: Invasive Carcinoma; DC: Ductal Carcinoma; NSC: Non-specific Carcinoma; SC: Sarcoma Carcinoma; MC: Mixed Carcinoma; PC: Phyllodes Carcinoma; CRC: Cribiform Carcinoma
Table 2: Distribution of biological subtypes
|
Phenotype |
HER2+ |
Luminal A |
Luminal B |
Triple negative |
RP+ RE- HER2+ |
RP+ RE- HER2- |
| Number |
3 |
22 |
11 |
12 |
1 |
1 |
| Frequency |
6 |
44 |
22 |
24 |
2 |
2 |
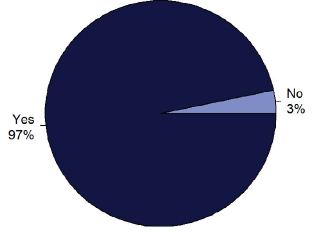
Figure 4: Patient mortality distribution. Yes: alive; No: dead
The results are shown in Figures 5-10. Patients who smoked had more grade III tumors. In addition, age was significantly correlated with disease stage (p=0.047) and molecular classification (p=0.0011).
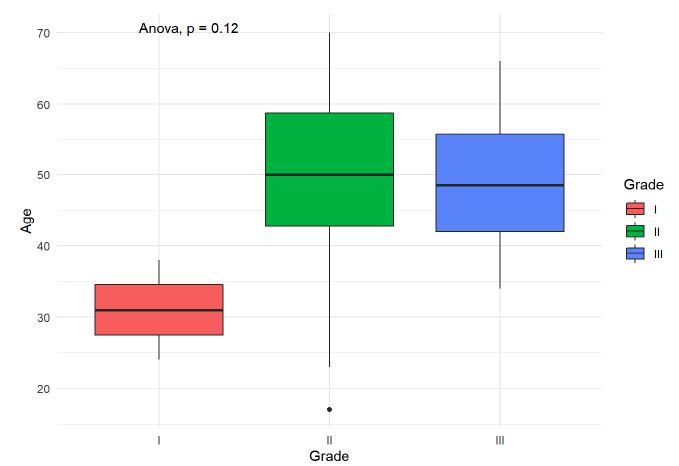
Figure 5: Correlation between age and grade
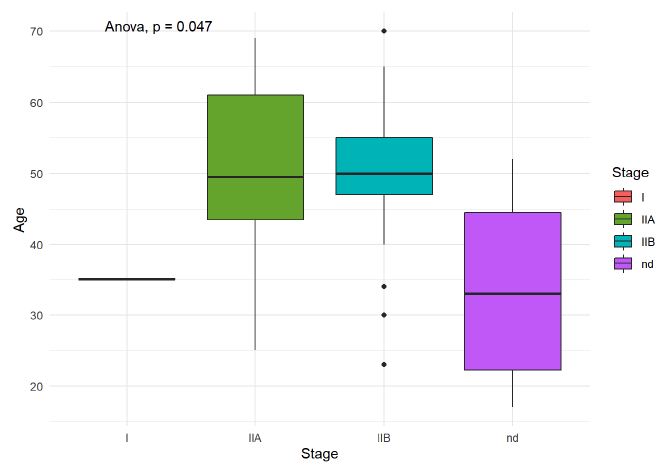
Figure 6: Correlation between age and stage
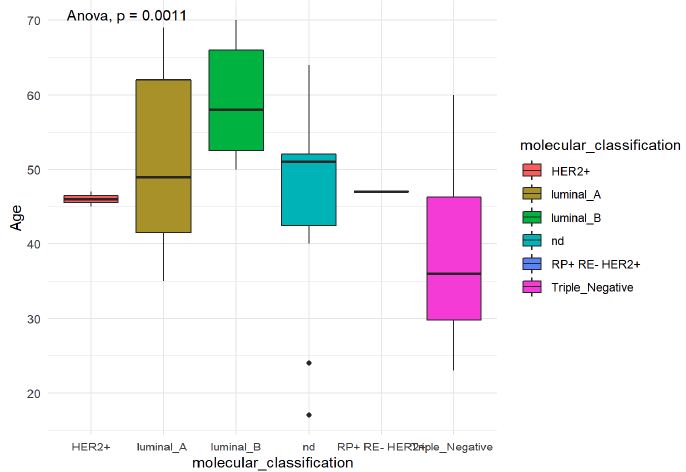
Figure 7: Correlation between age and molecular classification
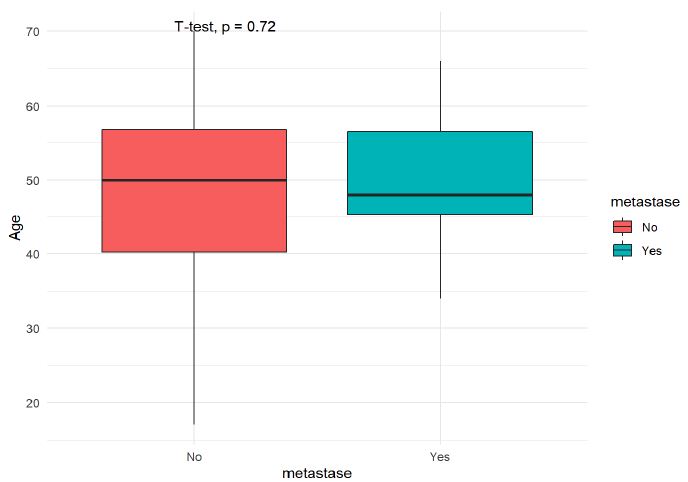
Figure 8: Correlation between age and presence of metastasis
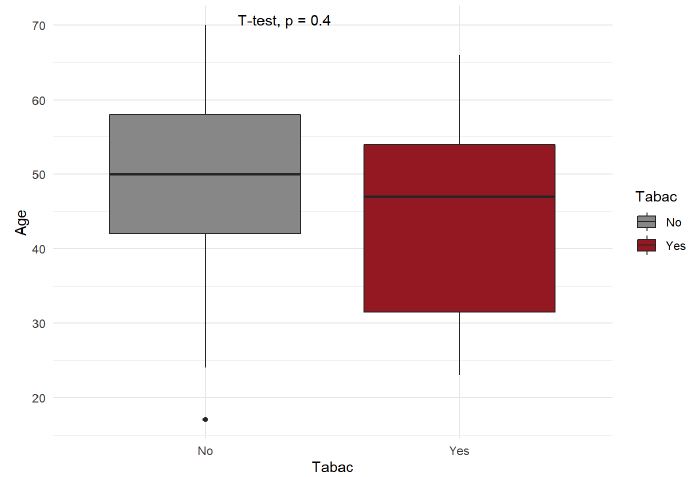
Figure 9: Correlation between age and tobacco consumption
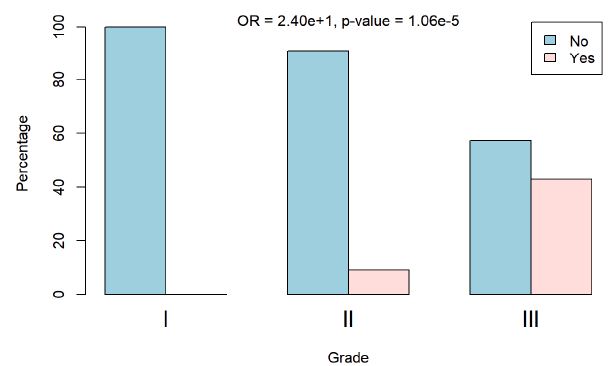
Figure 10: Histological grade according to tobacco consumption
Discussion
We enrolled 60 patients with newly diagnosed breast cancer. The 40-50 age group accounts for 36.66% of women affected by this pathology. The median age at the time of diagnosis was 48.71 years. This does conflicts with the data obtained in France (mean age: 61 years) [6], and in Algeria (average age: 50 years) [5]. The average age at menarche was 12.66 years in this study. The literature data are consistent with those of our study; we found that more than half (58.33%) of our patients had their first period at ≤12 years, and puberty before 12 years is known to increase the risk of breast cancer in adulthood through longer exposure to estrogen. The incidence of nulliparity was low in the present study. However, our patients were not multiparous and the majority (71.66%) only had one child. However, a higher number of children appeared to have a protective effect [7].
Breast cancer diagnoses often occur at a late stage, which could be due to insufficient health education and the poor socioeconomic status of the population. Of our patients, 16.66% were in a metastatic stage at the time of diagnosis. Considering these factors, it is clear that screening and awareness campaigns should be launched and strengthened to help resolved these problems. Of the patients, 93.33% discovered the disease through self-examination of a nodule. In 58.33% of cases, the tumor involved the right breast. The predominance of cancer in one breast over the other can be explained by breastfeeding habits [8]. In the literature, breast cancer is generally unilateral and rarely affects both the breasts. This was confirmed by our study, in which bilateral localization representing only 5%.
A relatively high number of young patients experience additional problems in terms of care. Indeed, several studies [9-12] have reported that breast cancer in young women tends to be more aggressive with a higher frequency of grade III SBR classification and negative estrogen receptors; in our study 20% of the patients were young (<40 years). Measurement of tumor size, both clinically and macroscopically, is an important prognostic element for therapeutic management. In our series, we noticed a slight decrease in advanced T3 and T4 forms compared to the results found in the studies by Mesmoudi [13] and Marrakech [14]. The T2 form was the most common (74.98%). The histological type was identified in all patients; invasive epithelial tumors were the most frequent, with infiltrating ductal carcinoma occurring in 70% of the cases.
Many studies have established that patients with locoregional metastases have poorer prognoses than those without lymph node involvement. Overall, ten-year survival is 70% when there is no lymph node involvement, and 25-30% in the presence of neoplastic invasion of the lymph nodes [15]. In our series, 96.66% of patients had lymph node invasion, and an average of two nodes were affected. All studies showed that metastatic risk and survival are strongly correlated with grade, regardless of the grading system used, and SBR grade III was associated with poorer prognosis than grades I and II. In the present study, grade II tumors had a predominance of 73.33%. Hormonal estrogen receptors are markers of tumor differentiation, whereas progesterone receptor positivity reflects the functionality of estrogen receptors. Hormonal receptors are prognostic factors because their expression is an indicator of good prognosis and is especially predictive of the response to hormone treatment [16]. Hormone receptors were studied in our patients, and 24% were triple negative.
Conclusion
Late diagnosis continues to worsen the prognosis for this cancer. The other findings in terms of epidemiological, clinical, and histopathological aspects were similar to those of previous studies in developing countries. Through this study, we concluded the following: 1) the rate of tumors diagnosed at a late stage remains relatively high; 2) the rate of tumors with a high histoprognostic grade and histological lymph node invasion remains significant; 3) invasive epithelial tumors are the predominate type of breast cancer. Breast cancer remains a serious pathology that is difficult to overcome, and its management remains hindered by socioeconomic conditions; therefore, a screening policy at a cost affordable to the population should be implemented and the awareness campaigns should be continued.
References
- Parkin DM, Whelan SL, Ferlay J, Teppo L, et al. (2002) Cancer Incidence in Five Continents: Volume VIII. Lyon: International Agency for Research on Cancer 155. [crossref]
- Ferlay J, Ervik M, Lam F, Colombet M, et al. (2020) Global Cancer Obser-Vatory: Cancer Today. International Agency for Research on Cancer; Lyon, France.
- Baba ND, Sauvaget C (2013) Le cancer en Mauritanie: résultats sur 10 ans du registre hospitalier de Nouakchott. Pan Afr Med J 14: 149. [crossref]
- Mohamed S (2017) Étude Épidémiologique de cancers en Mauritanie. Mémoire de Master Université de Nouakchott AL Asriya.
- Bouzbid S, Aouras H, Djeddi H, Yassi F (2014) Le cancer du sein chez la femme dans le département d’Annaba, Algérie. Revue d’Épidémiologie et de Santé Publique 62: S215.
- World Health Organization. Morocco: Incidence, Mortality and Prevalence by cancer site. Globocan 2018. Accessed 23 November 2019.
- Pathak DR, Speizer FE, Willet WC, Rosner B, et al. (1986) Parity and breast cancer risk: possible effect on age at diagnosis. Int J Cancer 37: 21-25. [crossref]
- Bonafos M, De Canelier R (1971) Cancers génitaux de la femme algérienne. Revue Afrique Noire 18: 235-240.
- Bakkali H, Marchal C, Lesur-Schwander J, Verhaeghe L (2003) Le cancer du sein chez la femme de 30 ans et moins. Cancer/radiothérapie 7: 153-159.
- Tabbane F, El May A, Hachiche M, Bahi J, et al. (1985) Breast cancer in women under 30 years of age. Breast Cancer Res Treat 6: 137-144.
- Althuis MD, Brogan DD, Coates RJ, Daling JR, et al. (2003) Breast cancers among very premenopausal women (United States). Cancer Causes Control 14: 151-160. [crossref]
- De Jesus MA, Fujita M, Kim KS, Goldson AL (2003) Retrospective analysis of breast cancer among young African American females. Breast Cancer Res Treat 78: 81-87. [crossref]
- Menikhar I (2017) Cancer du sein étude rétrospective à propos de 270 cas au CHU Ibn-Rochd de Casablanca. Casablanca-Maroc. Faculté de médecine et de pharmacie de Casablanca.
- Bouaalloucha S (2012) Le profil épidémiologique et clinique du cancer du sein chez la femme au CHU Mohammed VI de Marrakech. Marrakech- Maroc. Faculté de médecine et de pharmacie Marrakech.
- Galant C, Berliere M, Leconte I, Marbaix E (2010) Nouveautés dans les facteurs histopronostiques des cancers du sein. Imag. de la Femme 20: 9-17.
- Moise N, Hery M, Serin D, Spielmann M (2005) Cancer du sein: Compte-rendu du cours supérieur francophone de cancérologie. Saint Paul de Vence: Springer Paris. [crossref]